

A version of this post appeared in the Austin-American Statesman
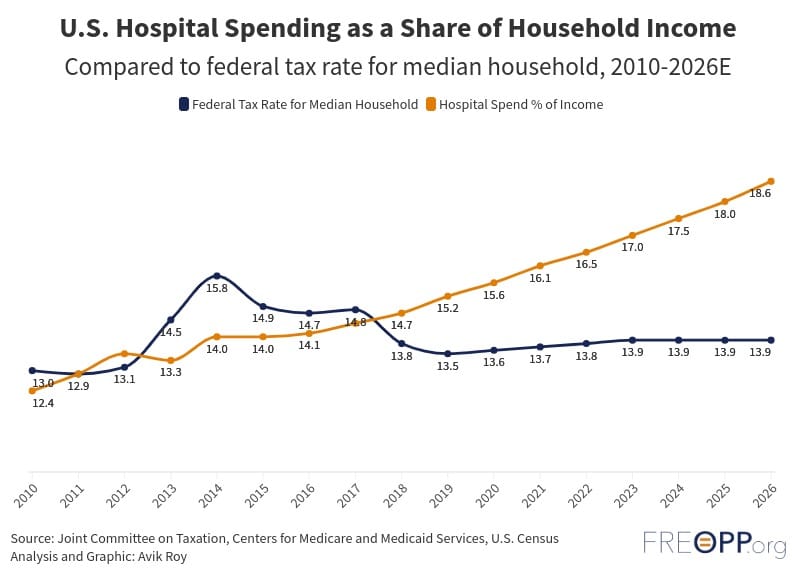
Hospital care is a driving force behind skyrocketing health care costs across the nation, including here in Texas. Hospital bills are so high that the average American family now pays more to hospitals than they pay in federal income and payroll taxes.
The United States pays more for hospital care than any other nation, despite using hospital services less frequently. In short, Americans pay more for hospital care because prices are higher than anywhere in the world.
One of the glaring ways hospitals overcharge patients is by charging more for care in hospital-owned physician’s clinics. For instance, a doctor that performs a routine test in a hospital-owned clinic charges an additional “facility fee” above what would be charged if the test was performed in an independently owned doctor’s office.
For decades, our convoluted health care system has allowed providers to bill different amounts for services based on the location where they are performed. Not only does this increase the cost of care, but it also incentivizes hospitals to acquire physicians’ practices so the hospital has more opportunities to add such fees. As hospitals swallow up more practices, lucrative facility fees become commonplace, fueling more consolidation in a vicious cycle. Facility fees are now so ingrained in hospital billing practices that providers have even charged them when their doctors perform telehealth visits, when no facility is required.
Eliminating the ability of hospitals to charge a higher rate for the same office-based care—a reform known as site-neutral payment—would reduce health care costs without affecting care quality.
For instance, Congress recently introduced the Facilitating Accountability in Reimbursement (FAIR) Act in the House and the Site-based Invoicing and Transparency Enhancement (SITE) Act in the Senate. These bills would prevent hospital-owned clinics from charging facility fees. Additionally, health reform bills like the Fair Care Act, sponsored by Arkansas Rep. Bruce Westerman and Indiana Sen. Mike Braun, include site-neutral payment reforms alongside other attempts to reduce consolidation in local hospital markets. The Hospital Competition Act, sponsored by Indiana Rep. Jim Banks, incentivizes monopoly hospital systems to divest ownership of subsidiaries to reintroduce local competition.
Eliminating facility fees for services performed in physician office settings would save billions for patients and taxpayers. For instance, the SITE Act would reduce the federal budget deficit by up to $117 billion over ten years and slash overall national health care expenditures by up to $458 billion, according to a projection from the Committee for a Responsible Federal Budget.
Unsurprisingly, the hospital lobby opposes attempts to implement site-neutral payment. Hospitals wield considerable political power in Washington, convincing many politicians that any policy that reduces hospital revenue—including site-neutral payment—will cause hospitals to go bankrupt. But under this logic, policymakers should allow hospitals to acquire every physician practice to charge higher prices for office-based services, even though independent practices consistently offer them at a lower price. Instead, hospitals should get out of the business of offering services that others could provide at a lower cost, and instead focus on providing more intensive services that only they can provide.
More importantly, we simply can no longer accept the crushing weight of hospital bills on patients and families, especially those at or below median income. Site-neutral billing reforms, like those included in the Fair Care Act, the FAIR Act, and the SITE Act, are essential to relieve the health care cost burdens of hardworking Texans. These bills represent a chance to break free from the shackles of outdated hospital billing practices, fostering an environment where health care is driven by the needs of patients, not the location of service delivery.
